Graham Hughes, who first described antiphospholipid syndrome (APS) in 1983, urged for more efforts to raise awareness of this disorder. APS often remains undiagnosed and untreated with catastrophic consequences, such as multiple miscarriages, or stroke at a young age.
Clinical features of APS
Clinical manifestations of antiphospholipid syndrome (APS) include:
- venous, arterial, and small-vessel thrombosis
- pregnancy loss
- preterm delivery for patients with severe pre-eclampsia or placental insufficiency
- cardiac valvular disease
- renal thrombotic microangiopathy
- thrombocytopenia
- haemolytic anaemia
- cognitive impairment
Antibodies
Antiphospholipid antibodies promote activation of endothelial cells, monocytes, and platelets; and overproduction of tissue factor and thromboxane A2 (procoagulants). Complement activation might have a central pathogenetic role.
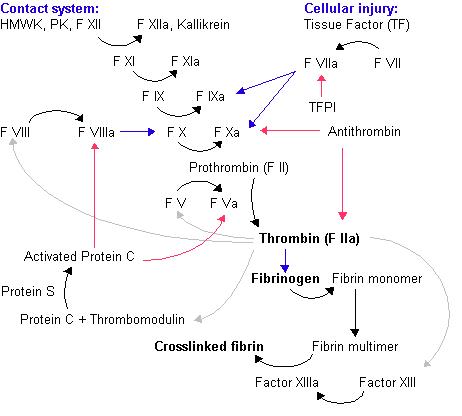
The coagulation cascade. Black arrow - conversion/activation of factor. Red arrows - action of inhibitors. Blue arrows - reactions catalysed by activated factor. Grey arrow - various functions of thrombin. Image source: Wikipedia
Of the different antiphospholipid antibodies, lupus anticoagulant is the strongest predictor of clinical presentation.
Treatment of APS
Therapy of thrombosis is based on long-term oral anticoagulation (warfarin). Patients with arterial events should be treated aggressively.
Primary thromboprophylaxis is recommended in patients with systemic lupus erythematosus (SLE) and in obstetric antiphospholipid syndrome. Obstetric care is based on treatment with aspirin and heparin.
Hydroxychloroquine is a potential additional treatment for APS. Possible future therapies for non-pregnant patients with antiphospholipid syndrome are statins, rituximab, and new anticoagulant drugs.
References
References
Antiphospholipid syndrome. The Lancet, Volume 376, Issue 9751, Pages 1498 - 1509, 30 October 2010.
Raising awareness of antiphospholipid antibody syndrome. The Lancet, Volume 375, Issue 9717, Page 778, 6 March 2010.