Friday, April 30, 2010
Should Doctors ‘Prescribe’ a Drink a Day? No.
 From the NYTimes:
From the NYTimes:The evidence regarding wine versus other beverages like grape juice is mixed.For most people, low-risk drinking is not harmful to health — and may be helpful. However, I would discourage people from drinking in order to improve their health.
Compared with non-drinkers, men who consumed wine, beer, or spirits had a 36% lower risk of all-cause mortality and a 34% lower risk of cardiovascular mortality.
Before you recommend wine for cardiovascular risk reduction, consider this:
- One in five men at risk of drinking problem during their lifetimes
- Women have an 8 to 10 percent chance of becoming dependent on alcohol during their lifetimes
- Men have 15% lifetime risk for alcohol abuse, 10% risk for alcohol dependence. Each cuts your life short by 10-15 years.
- Heavy drinking increases risk of depression by 40%, and 80% of people dependent on alcohol are smokers
Alcohol literally kills: Gary Moore had 380mg/dL in his blood, Winehouse 416mg/dL when she died surrounded by 3 empty vodka bottles. Telegraph UK, 2012.
Alcohol literally kills: Gary Moore had 380mg/dL in his blood, Winehouse 416mg/dL when she died surrounded by 3 empty vodka bottles. Telegraph UK, 2012.
References:
Should Doctors ‘Prescribe’ a Drink a Day? NYtimes, 2010.
Before you recommend wine for CV risk reduction, consider this: 1 in 5 men at risk of drinking problem
Rethinking Drinking - NIH interactive website
Image source: Wikipedia, public domain.
Comments from Twitter:
OMC @charlesayanleke: That's a recommendation most peeps can get behind
Tibor Banyai @tibor75: Do u tell your AF pts to be 100% abstinent? Curious RT @drjohnm: RT @DrVes: Should Doctors ‘Prescribe’ a Drink a Day? No.
John Mandrola, MD @drjohnm: No I don't rec abstinence but I don't feel that alcohol adds to health. Mild intake prob neutral. Worry about cancer risk
Rethinking Drinking - NIH interactive website
Image source: Wikipedia, public domain.
Comments from Twitter:
OMC @charlesayanleke: That's a recommendation most peeps can get behind
Tibor Banyai @tibor75: Do u tell your AF pts to be 100% abstinent? Curious RT @drjohnm: RT @DrVes: Should Doctors ‘Prescribe’ a Drink a Day? No.
John Mandrola, MD @drjohnm: No I don't rec abstinence but I don't feel that alcohol adds to health. Mild intake prob neutral. Worry about cancer risk
Thursday, April 29, 2010
High deductible health insurance can be bad for your health
 See why:
See why:"The individual health insurance policy they bought to replace Janie's group coverage at work has such a high deductible that they've sharply cut back doctor visits, skipping some routine care and going only when absolutely necessary.
Freelancers Janie and Chris Peterson love the freedom of life without a boss. But it comes with a high price -- dwindling savings, erratic cash flow, and a ton of financial anxiety."
References:
Financial planning for freelance workers - Mar. 11, 2010. CNN.
Image source: United States one-dollar bill. Wikipedia, public domain.
{kind=link}
Wednesday, April 28, 2010
"The doctor in literature: Private life" by Solomon Posen at Google Books
"This is a structured, annotated and indexed anthology dealing with the personality and the behaviour of doctors, and doctor-patient relationships - ideal for medical humanities courses."
Medical school letters of recommendation have formally been replaced by tweets

Doctor_V's tweets in Brizzly (click to enlarge the image) - read from the bottom of the screenshot.
If you are a medical school I highly suggest you admit @beccacamp .@LeeAase I don't know if Mayo School of Medicine takes Twitter recommendations but I formally recommend @beccacamp. Medical school letters of recommendation have formally been replaced by tweets.
Indeed. And if the tweets are by Doctor_V, they should be strongly considered in the admission process... :)
Tuesday, April 27, 2010
The men behind famous eponymous diseases
From CNN:
"Having a disease named after you is a decidedly mixed bag. On the one hand, your scientific developments are forever commemorated. On the other hand, though, you're stuck with the knowledge that no patient will ever be happy upon hearing your name."

Daniel Elmer Salmon (1850 – 1914) was a veterinary surgeon. He earned the first D.V.M. degree awarded in the United States, and spent his career studying animal diseases for the U.S. Department of Agriculture. He gave his name to the Salmonella genus of bacteria, which were discovered by an assistant, and named in his honor. Image source: Wikipedia, public domain.
New medical conditions that are being discovered are not named after scientists or physicians anymore. The eponymous system is non-descriptive and generally confusing.
References:
"Having a disease named after you is a decidedly mixed bag. On the one hand, your scientific developments are forever commemorated. On the other hand, though, you're stuck with the knowledge that no patient will ever be happy upon hearing your name."
Daniel Elmer Salmon (1850 – 1914) was a veterinary surgeon. He earned the first D.V.M. degree awarded in the United States, and spent his career studying animal diseases for the U.S. Department of Agriculture. He gave his name to the Salmonella genus of bacteria, which were discovered by an assistant, and named in his honor. Image source: Wikipedia, public domain.
New medical conditions that are being discovered are not named after scientists or physicians anymore. The eponymous system is non-descriptive and generally confusing.
References:
Monday, April 26, 2010
3-gram reduction in daily salt intake would decrease coronary heart disease, stroke, and death
 The U.S. diet is high in salt, with the majority coming from processed foods. Reducing dietary salt is a potentially important target for the improvement of public health.
The U.S. diet is high in salt, with the majority coming from processed foods. Reducing dietary salt is a potentially important target for the improvement of public health.Reducing dietary salt by 3 g per day (1200 mg of sodium per day) is projected to reduce the annual number of new cases of CHD by 60,000 to 120,000, stroke by 32,000 to 66,000, and myocardial infarction by 54,000 to 99,000 and to reduce the annual number of deaths from any cause by 44,000 to 92,000. Such an intervention would be more cost-effective than using medications to lower blood pressure in all persons with hypertension.
The cardiovascular benefits of reduced salt intake are on par with the benefits of population-wide reductions in tobacco use, obesity, and cholesterol levels.
References:
Projected Effect of Dietary Salt Reductions on Future Cardiovascular Disease. NEJM, 2010.
http://content.nejm.org/cgi/content/short/362/7/590
Sweat Bees prefer sweaty people because the human diet is so salty that their perspiration is saturated with that essential nutrient. WSJ, 2012.
Image source: Single-serving salt packets. Wikipedia, GNU Free Documentation License.
{kind=link}
Fish out of pills - Pharmaceuticals in drinking water
Fish out of pills - Pharmaceuticals in drinking water, NationalGeographic, April 01, 2010. Design Editor Oliver Uberti shows what went into the making of an information graphic about pharmaceuticals that make their way into our watersheds and end up in fish. Click here to see the full-size illustration.
A vast array of pharmaceuticals — including antibiotics, anti-convulsants, mood stabilizers and sex hormones — have been found in the drinking water supplies of at least 41 million Americans. The concentrations of these pharmaceuticals are tiny, far below the levels of a medical dose but the long-term consequences to human health are unknown.
The pharmaceutical industry points out the amount of medication in the water supply is the equivalent of a single pill in an Olympic-size swimming pool. Still, if you a have glass of water in Philadelphia, you are drinking tiny amounts of at least 56 medications.
Antibiotics, anticonvulsants, antidepressants and sex hormones in drinking water of 41 million Americans http://goo.gl/HiXa
AP Probe Finds Drugs in Drinking Water. Associated Press.
Drugs in water causing troubling problems to fish, wildlife. CNN.
In U.S., bottled water lacks drug safeguards. CNN.
Pollution: Fish Pharm. NGM Blog Central.In U.S., bottled water lacks drug safeguards. CNN.
Fishing For Answers: How To Choose Fish and Seafood | Summer Tomato http://goo.gl/0OBf
Something in the water - fluoxetine in this river, antihypertensives in that lake - BMJ, 2011.
Something in the water - fluoxetine in this river, antihypertensives in that lake - BMJ, 2011.
Sunday, April 25, 2010
FDA: High-dose simvastatin increases risk of muscle injury - caution with lower doses plus Amiodarone, Verapamil, Diltiazem
 Based on review of data from a large clinical trial and data from other sources, the U.S. Food and Drug Administration (FDA) is informing the public about an increased risk of muscle injury in patients taking the highest approved dose of the cholesterol-lowering medication, Zocor (simvastatin) 80 mg, compared to patients taking lower doses of simvastatin and possibly other drugs in the "statin" class.
Based on review of data from a large clinical trial and data from other sources, the U.S. Food and Drug Administration (FDA) is informing the public about an increased risk of muscle injury in patients taking the highest approved dose of the cholesterol-lowering medication, Zocor (simvastatin) 80 mg, compared to patients taking lower doses of simvastatin and possibly other drugs in the "statin" class.The muscle injury, also called myopathy, is a known side effect with all statin medications. The most serious form of myopathy is called rhabdomyolysis. Patients with myopathy generally have muscle pain, tenderness or weakness, and an elevation of a muscle enzyme in the blood (creatine kinase). The higher the dose of statin used, the greater the risk of developing myopathy. The risk of myopathy is also increased when simvastatin, especially at the higher doses, is used with certain drugs (see Simvastatin Dose Limitations below).
The data come from the SEARCH study, in which myopathy was seen in nearly 1% of patients taking the 80 milligram dose of Zocor but in only 0.02% of patients taking the 20 milligram dose of Zocor.
Update 6/2011: FDA Restricts Use of Simvastatin 80 mg, due to increased risk of muscle damage http://goo.gl/K9O5v
Rhabdomyolysis was rare in the SEARCH study. It happened in only 11 of 6,031 patients (0.02%) in group taking the 80 milligram dose of Zocor, but was not seen in patients taking the 20 milligram dose.
New data also suggest that people of Chinese descent should not take Zocor at the 80 milligram dose -- and should be careful even when taking lower doses -- if they also take niacin-containing products.
Simvastatin Dose Limitations
These limitations apply to ALL patients taking simvastatin.
Do not use simvastatin with these medications:
Itraconazole
Ketoconazole
Erythromycin
Clarithromycin
Telithromycin
HIV protease inhibitors
Nefazodone
Do not use more than 10mg of simvastatin with these medications:
Rhabdomyolysis was rare in the SEARCH study. It happened in only 11 of 6,031 patients (0.02%) in group taking the 80 milligram dose of Zocor, but was not seen in patients taking the 20 milligram dose.
New data also suggest that people of Chinese descent should not take Zocor at the 80 milligram dose -- and should be careful even when taking lower doses -- if they also take niacin-containing products.
Simvastatin Dose Limitations
These limitations apply to ALL patients taking simvastatin.
Do not use simvastatin with these medications:
Itraconazole
Ketoconazole
Erythromycin
Clarithromycin
Telithromycin
HIV protease inhibitors
Nefazodone
Do not use more than 10mg of simvastatin with these medications:
Gemfibrozil
Cyclosporine
Danazol
Do not use more than 20mg of simvastatin with these medications:
Cyclosporine
Danazol
Do not use more than 20mg of simvastatin with these medications:
Amiodarone
Verapamil
Do not use more than 40mg of simvastatin with this medication:
Verapamil
Do not use more than 40mg of simvastatin with this medication:
Diltiazem
References:
References:
FDA Drug Safety Communication: Ongoing safety review of high-dose Zocor (simvastatin) and increased risk of muscle injury. FDA.
FDA Warns of Zocor Risk to Muscles. WebMD.
FDA Warns of Zocor Risk to Muscles. WebMD.
FDA Restricts Use of Simvastatin 80 mg, due to increased risk of muscle damage http://goo.gl/K9O5v
Image source: Simvastatin. Wikipedia, public domain.
{kind=link}
Saturday, April 24, 2010
Occupation may be a key factor in lung cancer
While cigarettes are by far the most important cause of lung cancer, chemicals and other on-the-job hazards "play a remarkable role" in lung cancer risk.
5% of lung cancers in men are job-related. Men in the known to be risky occupations were 74% more likely to have been diagnosed with lung cancer.
The strongest associations were seen for ceramic and pottery jobs and brick manufacturing, as well as for those working in manufacturing of non-iron metals.
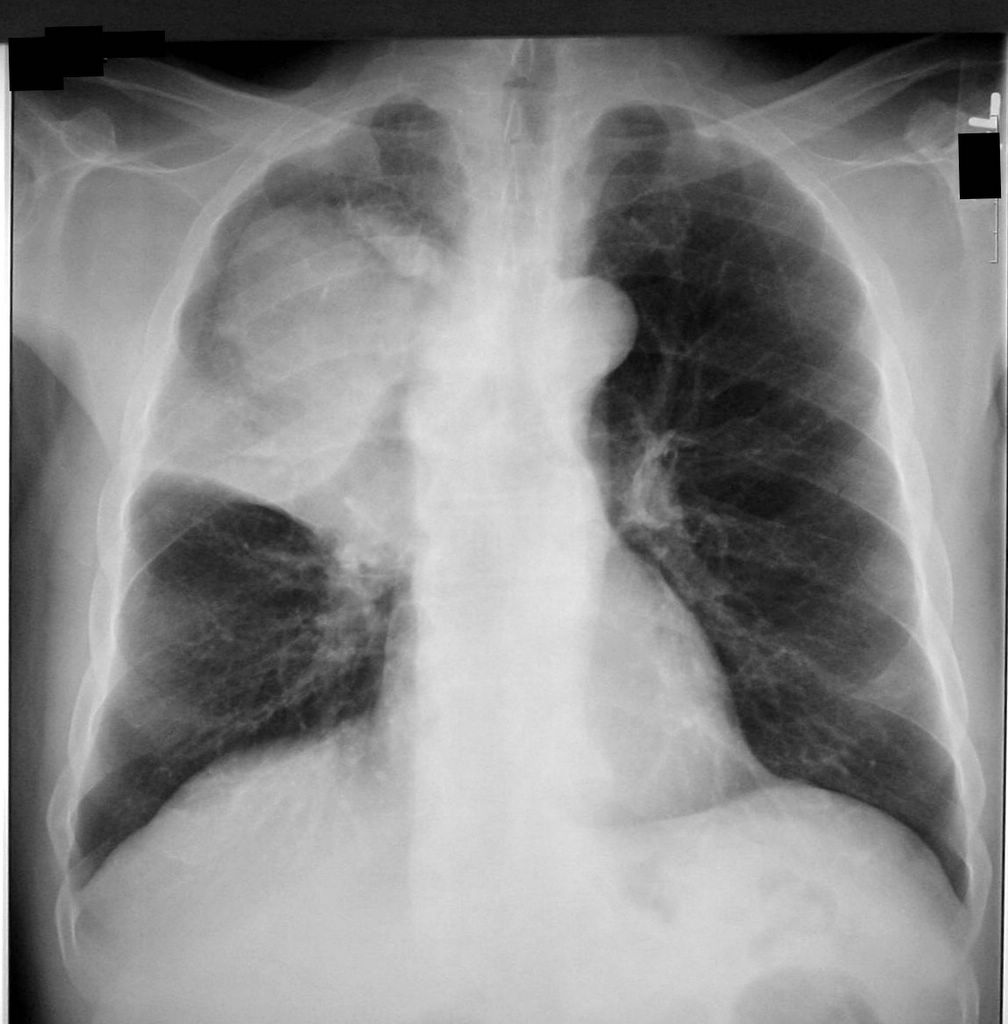 A CXR shows a right upper lobe (RUL) mass due to lung cancer. Source: Finger Clubbing due to Lung Cancer. Clinical Cases and Images.
A CXR shows a right upper lobe (RUL) mass due to lung cancer. Source: Finger Clubbing due to Lung Cancer. Clinical Cases and Images.
References:
5% of lung cancers in men are job-related. Men in the known to be risky occupations were 74% more likely to have been diagnosed with lung cancer.
The strongest associations were seen for ceramic and pottery jobs and brick manufacturing, as well as for those working in manufacturing of non-iron metals.
References:
Occupation a key factor in men's lung cancer risk. Reuters, 2010.
http://www.reuters.com/article/idUSTRE61E53920100215
http://www.reuters.com/article/idUSTRE61E53920100215
Friday, April 23, 2010
Hockey-puck-on-a-rod test checks for concussion after head trauma
 From NPR:
From NPR:The hockey-puck-on-a-rod test was invented by a Michigan high school student.
It works like this: Tester suspends the device while injured athlete sits with forearm on table, fingers loosely circling the stick. Without warning, tester drops stick. Athlete grabs stick as fast as possible. Place where athlete grabs gives an instant readout of reaction time.
It all happens in milliseconds - too fast to measure with a stopwatch. Athletes with concussions had reaction times that were 15% slower.
References:
Comments:
Nicholas Genes - Neat idea. I like how it's free of stopwatches and all the variability they introduce. But it seems that athletes would need to have a baseline measurement pre-trauma to really compare (maybe they can do it when they're signing waivers at the start of the season...)
Thursday, April 22, 2010
Rock legend Ronnie James Dio is fighting stomach cancer
On 25 November 2009, Dio's wife and manager announced that he was diagnosed with stomach cancer:
"Ronnie has been diagnosed with the early stages of stomach cancer. We are starting treatment immediately at the Mayo Clinic. After he kills this dragon, Ronnie will be back on stage, where he belongs, doing what he loves best, performing for his fans. Long live rock and roll, long live Ronnie James Dio. Thanks to all the friends and fans from all over the world that have sent well wishes. This has really helped to keep his spirit up." -- "He has had a few hiccups between Christmas and New Year's," she said in a statement to fans. "He has had a blood clot, a trip to the emergency room, and a three-day stay at the hospital."
ArtisanNewsService — April 13, 2010 — "One of heavy metal's premiere vocalists Ronnie James Dio shares his thoughts on his battle with stomach cancer at the Revolver Golden Gods awards."
On 14 March 2010, Dio's wife and manager Wendy posted an online update on his condition:
"It has been Ronnie's 7th chemo, another cat scan and another endoscopy, and the results are good - the main tumour has shrunk considerably, and our visits to Houston (MD Anderson Cancer Center in Texas) are now every three weeks instead of every two weeks."
"Ronnie has been diagnosed with the early stages of stomach cancer. We are starting treatment immediately at the Mayo Clinic. After he kills this dragon, Ronnie will be back on stage, where he belongs, doing what he loves best, performing for his fans. Long live rock and roll, long live Ronnie James Dio. Thanks to all the friends and fans from all over the world that have sent well wishes. This has really helped to keep his spirit up." -- "He has had a few hiccups between Christmas and New Year's," she said in a statement to fans. "He has had a blood clot, a trip to the emergency room, and a three-day stay at the hospital."
ArtisanNewsService — April 13, 2010 — "One of heavy metal's premiere vocalists Ronnie James Dio shares his thoughts on his battle with stomach cancer at the Revolver Golden Gods awards."
On 14 March 2010, Dio's wife and manager Wendy posted an online update on his condition:
"It has been Ronnie's 7th chemo, another cat scan and another endoscopy, and the results are good - the main tumour has shrunk considerably, and our visits to Houston (MD Anderson Cancer Center in Texas) are now every three weeks instead of every two weeks."
Ronnie James Dio passed away on May 16, 2010 at age 67. The music lives on: http://www.ronniejamesdio.com
References:
Ronnie James Dio. Wikipedia.
Black Sabbath, Dio singer Ronnie James Dio gives cancer update. NME.com.
References:
Ronnie James Dio. Wikipedia.
Black Sabbath, Dio singer Ronnie James Dio gives cancer update. NME.com.
Metal legend Ronnie James Dio dead at 67. USA Today, 2010.
Ronnie James Dio, Rock Singer, Dies at 67. NYTimes, 2010.
Ronnie James Dio died at age 67. YouTube.
Ronnie James Dio Remembered By Metallica's Lars Ulrich. MTV.
The Lighter Side of Ronnie James Dio. NYTimes.
Lars Ulrich's letter to Dio.
Ronnie James Dio, Rock Singer, Dies at 67. NYTimes, 2010.
Ronnie James Dio died at age 67. YouTube.
Ronnie James Dio Remembered By Metallica's Lars Ulrich. MTV.
The Lighter Side of Ronnie James Dio. NYTimes.
Lars Ulrich's letter to Dio.
Dio, another day. Nigel Britto, TOI Crest, May 22, 2010.
Dio monument in Bulgaria - source one, two, three (in Bulgarian), 10/2010.
Dio monument in Bulgaria - source one, two, three (in Bulgarian), 10/2010.
Updated: 10/24/2010
500 repetitions of 4 cardiac murmurs improved auscultatory proficiency of medical students
 According to a 2004 study in Chest, the ability of medical students to recognize heart murmurs is poor (20%), and does not improve with subsequent years of training.
According to a 2004 study in Chest, the ability of medical students to recognize heart murmurs is poor (20%), and does not improve with subsequent years of training.Five hundred repetitions of four basic cardiac murmurs significantly improved auscultatory proficiency in recognizing basic cardiac murmurs by medical students. These results suggest that cardiac auscultation is, in part, a technical skill.
Related resources
The Heart Sounds Tutorial by Blaufuss.org is a fancy flash-based simulator with animations. The McGill University Virtual Stethoscope is another useful website. Click here for more web-based teaching resources for hearts sounds from UCLA and breath sounds from Loyola University.
References:
Mastering cardiac murmurs: the power of repetition. Barrett MJ, Lacey CS, Sekara AE, Linden EA, Gracely EJ. Chest. 2004 Aug;126(2):470-5.
http://www.ncbi.nlm.nih.gov/pubmed/15302733 Image source: Modern stethoscope. Wikipedia, public domain.
{kind=link}
Wednesday, April 21, 2010
Standardized patient: Over the course of three days, I had 23 head-to-toe physicals from 23 medical students
 From Slate:
From Slate:"I was the first person these would-be doctors had ever fully examined on their own. Some were shaking so violently when they approached me with their otoscopes—the pointed device for looking in the ear—that I feared an imminent lobotomy.
A "standardized patient" is a trained person who is paid $15 an hour to be poked and prodded by inexperienced fingers, so that med students can learn communication and examination skills before they are sicced on actual sick people.
Now there are standardized patients trained for genital duty (they're called GUTAs, for genitourinary teaching associates).
Dr. N wasted the first eight minutes of the exam trying repeatedly to get a blood pressure reading. The panic in his eyes seemed to say, "She appears to be alive, yet she has no vital signs."
Comments:
Lakshman Swamy - Don't forget that some of them were capable! I have to say, in my experience as an MS2 at Wright State, our standardized patients are amazing teachers. It is much easier to learn physical exam skills and even interviewing when the patient can give you precise feedback. The author is right on with the characters that patients can portray... it is shocking when they break character to give feedback! Just recently I learned how to do the male exam with two standardized patients ("GUTA" -- never heard of that term before). I was definitely feeling a little ... awkward before the session began-- this was by far the most invasive thing I had ever done to another person. But the standardized patients were amazing about the whole process, even acting out the different hesitations that we might encounter in patients, emphasizing the importance of the exam, etc. Without being too graphic, I can't emphasize how much I learned about how to do those exams and what I was actually supposed to be finding. It was a totally different experience than I expected, and after it, I feel really confident about the whole process.
I can't even IMAGINE what it would be like to do that with my classmates-- and how much less I would have understood. Wow.
References:
Oh, no! I'm the first patient these 23 medical students have ever examined. Slate, 2010.
Image source: OpenClipArt.org, public domain.
Tuesday, April 20, 2010
AskaPatient.com - Medication Ratings and Health Care Opinions
 This website "reports patient ratings and rankings of pharmaceuticals and prescription drug side effects. Database includes FDA-approved pharmaceuticals."
This website "reports patient ratings and rankings of pharmaceuticals and prescription drug side effects. Database includes FDA-approved pharmaceuticals."http://www.askapatient.com
You can Search by Drug Name:
http://www.askapatient.com/rateyourmedicine.htm
You can add ratings for the medications you take or look at ratings and comments from other patients.
For example:
cetirizine
http://www.askapatient.com/viewrating.asp?drug=19835&name=ZYRTEC
simvastatin (scores rather low)
http://www.askapatient.com/viewrating.asp?drug=19766&name=ZOCOR
You can add ratings for the medications you take or look at ratings and comments from other patients.
For example:
cetirizine
http://www.askapatient.com/viewrating.asp?drug=19835&name=ZYRTEC
simvastatin (scores rather low)
http://www.askapatient.com/viewrating.asp?drug=19766&name=ZOCOR
Please note that I am not sure how useful the site is, and obviously, this post is not an endorsement or recommendation.
Related readings:
How reliable are those patient driven rating sites? Notes from Dr. RW, 2010.
Analysis of 4,999 Online Physician Ratings: most patients gave positive reviews (2011 study) http://goo.gl/LgG5L - It begs the question: couldn't researchers add 1 more for a round number 5,000?
Analysis of 4,999 Online Physician Ratings: most patients gave positive reviews (2011 study) http://goo.gl/LgG5L - It begs the question: couldn't researchers add 1 more for a round number 5,000?
Image source: AskaPatient.com.
Monday, April 19, 2010
Different types of kidney transplantation - Mayo Clinic video
"Dr. Raymond Heilman, Medical Director of the Kidney Transplant Program of Mayo Clinic in Arizona, gives an overview on the different types of kidney transplantation, including living donor and paired donor exchanges, and explains what kidney donors can expect."
The false idea that only the “top journals” publish the important stuff
 From the former Editor-in-Chief of BMJ:
From the former Editor-in-Chief of BMJ:The naïve concept that the “top journals” publish the important stuff and the lesser journals the unimportant is simply false. People who do systematic reviews know this well. Anybody reading only the “top journals” receives a distorted view of the world. Unfortunately many people, including most journalists, do pay most attention to the “top journals.”
References:
Richard Smith: Scrap peer review and beware of “top journals”. BMJ Blogs.
Google ranks the top 100 journals and NEJM is no more the "top dog" according to G Scholar Metrics for Publications http://goo.gl/unTjs
Comments from Google Buzz (March 22, 2010):
Heidi Allen - Love the fact that the BMJ have put out so bold a statement
Neil Mehta - Very provocative. Agree that Peer review is mostly a joke and a lottery. Unfortunately we still live in a world of publish or perish. We need to have something like a YouTube of papers. As more people read these and rate them, the cream will rise to the top. The raters should also be rated and that should also count towards academic promotion.
Lakshman Swamy - Neil-- I agree, but it should be a closed system. Anyone can read, but not anyone can rate-- have to have credentials of some sort. Can't risk creating another place for opinions to become stronger than data.
Ves Dimov, M.D. - On a more basic level, this is also a simple appeal to all physicians to read more than the top 5 journals. Wait... Most physician don't even read the top 5 journals.. :)
Social networks help in some way though - I tend to have a closer look at articles linked by the people I follow.
Vamsi Balakrishnan - @Neil Mehta A friend and myself actually shared that same idea about science, about publishing and its current state. We had a grandiose goal of starting a publishing site that would be more about sharing ideas than anything else (www.sciencetrader.com/).
When I think about publishing in famous journals being important, I think about the famous "cloner" who published in Nature (http://en.wikipedia.org/wiki/Hwang_Woo-Suk); if peer-review was successful, I doubt that he'd have been published his fabricated data. But, once you're successful and thus renowned, no one would have the courage to question you.
Kind of a similar situation is found with Einstein back in the day. When he was working on TOE (theory of everything; a unified grand scheme for how the universe works) he denied the possibility that quantum mechanics could rule the microcosm simply because of his belief that regardless of the evidence, "God does not play dice with the universe" (or something close to that). The macrocosm followed his rules exactly as he predicted, so the microcosm should do the same. No one questioned him since...it's Einstein. He's probably right. (He wasn't); I think Dr. Feynman said in his book (Surely You're Joking Dr. Feynman) it took another ~10 years before Einstein admitted he might be wrong...
Anyway, I diverge.
A last example that's more healthcare-related would be the scientist who developed valproic acid as a treatment for seizures. This scientist, Eymarde, made 30-40 drugs...every drug he made was GOLD, meaning they ALL worked. No one had as much success as he did in creating seizure medications. He could have said anything he wanted about seizures medications since he was the expert, and it was taken as the truth. Unlike most scientists out there though, he knew he was willing to admit that he's not perfect and that no one could make this many drugs work so well. So, he developed controlled studies...testing every component of the medication, only to find that the vector he used to dissolve his "drugs" in was the actual active component with anti-convulsive properties. A modern scientist...would not do anything. Publish or perish. If you just retracted every paper you've written for the last x amount of years...it'd be pretty hard to get future funding, even if you were being honest. This Eymarde did however respect his trade and his peers, so he retracted every one of his papers. After this bit of honest science, he was forgotten to the world and ridiculed.
In a completely circuitous way through three different example, I'm trying to say that I agree with you that peer review, and generally the scientific process now due to peer review is broken. Changes are needed.
Neil Mehta - Vamsi,
thanks for those examples. I was not familiar with the Einstein or the Eymarde examples - I want to publish my case series that suggests famous scientists with last names starting with E tend to make errors that they own up to several years later. Do you think that I should submit to top tier journals? Suggest Vamsi for peer review? Just kidding. Enjoyed reading your comments.
Look forward to more conversations
Vamsi Balakrishnan - Oh, wow, I didn't even notice the common endings. I went searching for a third "E" named person...but couldn't find one that is...on par with the Woo-Suk one.
If I write a book, it's going to be a collection of stories about famous scientists and the things that they...endured and the follies they've made.
It will be entitles, "Famous Scientists: The Things They Endured, and the Follies They've Made."
If I write a book, it's going to be a collection of stories about famous scientists and the things that they...endured and the follies they've made.
It will be entitles, "Famous Scientists: The Things They Endured, and the Follies They've Made."
Aidan Finley - http://www.nature.com/nature/history/timeline_1950s.html The Krebs Cycle paper was rejected by Nature for not being impactful.
http://www2.uah.es/jmc/ai56.pdf (article reviewing other major rejected discoveries, including the MRI). Nature editorial: http://www2.uah.es/jmc/
Ves Dimov, M.D. - "The Krebs Cycle paper was rejected by Nature for not being impactful."
Isn't this just amazing? Reality is truly stranger than fiction.... :)
Aidan Finley - To be fair, I think everyone recognizes it was a mistake.
Related reading:
Nature rejected/declined Krebs cycle paper in 1937 - there were too many submissions - but few remember them now... http://goo.gl/mcxPd
The grossest failures of peer review (PDF) http://goo.gl/3ovkn
Image source: 2009 cover of the journal BMJ, low resolution, fair use.
{kind=link}
Sunday, April 18, 2010
Mobile Medicine via iPod/iPhone/iPad Apps
NatureVideoChannel — March 31, 2010 — "You might not realize it, but with an iPhone, you also have a stethoscope and a CPR trainer within reach. These are just a few of the more than 2,000 medical applications available on the iPhone, and here we've rounded up ten for you to check out. Whether you're a researcher, doctor, or patient, get ready for your medicine to go mobile."
Smartphones and portable devices for medical education
I use an iPhone Touch to listen to lectures and watch presentations (PDF and video). Amazon Kindle works for the same purpose (PDF only, no video).
However, the external speaker of the iPhone Touch leaves much to be desired in terms of sound quality and volume, and recently, I started downloading the lectures directly to my cell phone (HTC Touch Pro2). The HTC Touch Pro interface is not as polished as the one on the iPod Touch but the device itself is not tied to iTunes and I can easily download audio files from the mobile sites of Google Reader, Bloglines and Google Docs.
Comments from Twitter:
@DrVes: Why are some doctors and nurses giving back their iPads? http://j.mp/Hq15aD - Easy: iPad works great for pt education, NOT for data entry. Only 10% of doctors currently use an iPad at work http://j.mp/Hq15aD - I use iPad daily to discuss these diagrams: http://j.mp/Hq1k5v
iPad is a great teaching tool @CraigCCRNCEN was able to explain to Vietnamese family AFib and clots by showing them animation from YouTube.
Brian S. McGowan PhD @BrianSMcGowan: so is the best option for docs still a touch screen laptop? teach w/ touch screen, work w/ full keyboard? #hcsm
@DrVes: iPad works well for discussing DDx, Tx options with pts. Much more portable than laptop. Full-keyboard COWs best for typing.
Jeff Bray @jeffkbray: I have been scanning all my medical reference books and store them on my iPad for quick use and no weight - great tool and mobile
Comments from Twitter:
@DrVes: Why are some doctors and nurses giving back their iPads? http://j.mp/Hq15aD - Easy: iPad works great for pt education, NOT for data entry. Only 10% of doctors currently use an iPad at work http://j.mp/Hq15aD - I use iPad daily to discuss these diagrams: http://j.mp/Hq1k5v
iPad is a great teaching tool @CraigCCRNCEN was able to explain to Vietnamese family AFib and clots by showing them animation from YouTube.
Brian S. McGowan PhD @BrianSMcGowan: so is the best option for docs still a touch screen laptop? teach w/ touch screen, work w/ full keyboard? #hcsm
@DrVes: iPad works well for discussing DDx, Tx options with pts. Much more portable than laptop. Full-keyboard COWs best for typing.
Jeff Bray @jeffkbray: I have been scanning all my medical reference books and store them on my iPad for quick use and no weight - great tool and mobile
Related:
Saturday, April 17, 2010
Better Sleep, Better Learning? Obstructive sleep apnea can reduce a child’s IQ by 10 points
 From Science Life Blog at the University of Chicago:
From Science Life Blog at the University of Chicago: Pediatric obstructive sleep apnea, or OSA, can have long-term, detrimental effects on a child’s cardiovascular and respiratory health. But it can also create neurocognitive effects, such as a reduced ability to learn and retain information.
OSA can reduce a child’s IQ by as many as 10 points, while treatment in children with OSA can improve grades.
References:
OSA can reduce a child’s IQ by as many as 10 points, while treatment in children with OSA can improve grades.
References:
Better Sleep, Better Learning? « Science Life Blog « University of Chicago.
http://sciencelife.uchospitals.edu/2010/02/15/better-sleep-better-learning
http://sciencelife.uchospitals.edu/2010/02/15/better-sleep-better-learning
Sleep duration is shorter in obese children http://goo.gl/z5JFs
Sleepiness and sleep-disordered breathing may be found in 19-29% of children with positive allergy test (http://goo.gl/AfCWZ).
Sleepiness and sleep-disordered breathing may be found in 19-29% of children with positive allergy test (http://goo.gl/AfCWZ).
Friday, April 16, 2010
Taking charge of your toddler's vaccination record is the best way to ensure they don't miss any shots
 From Reuters:
From Reuters:"In our country, we think the doctor should have all the medical records," said Dr. James McElligott, a pediatrician at the Medical University of South Carolina who worked on the study. "I like the idea of putting the ownership back in Mom's hands and empowering her a little bit."
When parents kept a so-called shot card, their child's odds of being up-to-date on vaccinations rose by more than half.
40 percent of the toddlers had a shot card, and 84 percent of these had up-to-date vaccinations. By contrast, only 79 percent of the children without a card had all their shots.
Use the card: it doesn't have a downside and it's cheap."
References:
Want kids' vaccinations up to date? Keep the record | Reuters, 2010.
http://www.reuters.com/article/idUSTRE61E37I20100215
http://www.reuters.com/article/idUSTRE61E37I20100215
The College of American Pathologists unveils a new patient website MyBiopsy.org
 The site is easy to navigate, well-organized and it looks helpful. Check the navigation menu in the left sidebar.
The site is easy to navigate, well-organized and it looks helpful. Check the navigation menu in the left sidebar.MyBiopsy.org redirects to:
http://www.cap.org/apps/docs/reference/myBiopsy/index2.html
RSS feed is also available: http://feeds2.feedburner.com/MybiopsyFeeds
This is the "fan page" on Facebook: http://www.facebook.com/MyBiopsy.org
(link via @Berci)
http://www.cap.org/apps/docs/reference/myBiopsy/index2.html
RSS feed is also available: http://feeds2.feedburner.com/MybiopsyFeeds
This is the "fan page" on Facebook: http://www.facebook.com/MyBiopsy.org
(link via @Berci)
Thursday, April 15, 2010
Vitamin D deficiency occurs frequently in COPD and correlates with severity
 Vitamin D is a steroid hormone and a component of a complex endocrine pathway sometimes called 'vitamin D endocrine system' (Medscape, 2012). 1 in 4 individuals will develop COPD during their lifetime (Lancet, 2011).
Vitamin D is a steroid hormone and a component of a complex endocrine pathway sometimes called 'vitamin D endocrine system' (Medscape, 2012). 1 in 4 individuals will develop COPD during their lifetime (Lancet, 2011).Serum 25-hydroxyvitamin D (25-OHD) levels were measured in 414 (ex)-smokers older than 50 years and the link between vitamin D status and presence of COPD was assessed. The rs7041 and rs4588 variants in the vitamin D-binding gene (GC) were genotyped and their effects on 25-OHD levels were tested.
In patients with COPD, 25-OHD levels correlated significantly with forced expiratory volume in 1 s (FEV1).
Compared with 31% of the smokers with normal lung function, as many as 60% and 77% of patients with GOLD (Global Initiative for Obstructive Lung Disease) stage 3 and 4 exhibited deficient 25-OHD levels lower than 20 ng/ml.
25-OHD levels were reduced by 25% in homozygous carriers of the rs7041 at-risk allele.
76% and 100% of patients with GOLD stage 3 and 4 homozygous for the rs7041 allele exhibited 25-OHD levels lower than 20 ng/ml.
Vitamin D deficiency occurs frequently in COPD and correlates with severity of COPD. The data warrant vitamin D supplementation in patients with severe COPD, especially in those carrying at-risk rs7041 variants.
Despite this circumstantial evidence, a recent trial of vitamin D replacement in patients with COPD did not show a reduction in exacerbations unless the patients had a severe vitamin D deficiency.
Vitamin D deficiency occurs frequently in COPD and correlates with severity of COPD. The data warrant vitamin D supplementation in patients with severe COPD, especially in those carrying at-risk rs7041 variants.
Despite this circumstantial evidence, a recent trial of vitamin D replacement in patients with COPD did not show a reduction in exacerbations unless the patients had a severe vitamin D deficiency.
References:
Vitamin D deficiency is highly prevalent in COPD and correlates with variants in the vitamin D-binding gene. Thorax 2010;65:215-220 doi:10.1136/thx.2009.120659.
http://thorax.bmj.com/content/65/3/215.short
A vitamin D3 dosage of 800 IU/d increased serum 25-(OH)D levels to greater than 50 nmol/L in 97.5% of women http://bit.ly/GzBCcA
A vitamin D3 dosage of 800 IU/d increased serum 25-(OH)D levels to greater than 50 nmol/L in 97.5% of women http://bit.ly/GzBCcA
Image source: Lungs, Wikipedia, public domain.
{kind=link}
Tools for Your Food Revolution - Wolfram|Alpha Lets You Compare Chicken to Corn Dog, Apple to Orange

Compare: chicken breast to corn dog
Compare: 1 apple to 1 orange
More comparisons:
Compare egg to cod
http://www.wolframalpha.com/input/?i=compare+egg+to+cod
Compare shrimp to cod
http://www.wolframalpha.com/input/?i=compare+shrimp+to+cod
References:
Wolfram|Alpha Blog : Tools for Your Food Revolution
http://blog.wolframalpha.com/2010/03/23/tools-for-your-food-revolution
The Personal Analytics of My Life - Stephen Wolfram Blog http://goo.gl/iwHRo
The Personal Analytics of My Life - Stephen Wolfram Blog http://goo.gl/iwHRo
Comments from Google Buzz:
I also like the simplicity of fealth
http://www.fealth.com/nutrition
Ves Dimov, M.D. - Looks interesting... I was not aware of Fealth... http://www.fealth.com/nutrition
Dr Mike Cadogan - Original post was here:
http://lifeinthefastlane.com/2008/09/physician-feed-thyself/
I think I will repost...
Ves Dimov, M.D. - Isn't it nice - the way a blog serves as a personal archive... I have not read the post either. Will have a look. Thank you for taking the time to review the service back in 2008.
Image source: Wikipedia, public domain.
{kind=link}
Wednesday, April 14, 2010
Nonsurgical Weight Loss with a Liquid Meal Program - Mayo Clinic Video
"Surgery may be an option for some people, but for those who don't want surgery or can't have it for medical reasons, there is another option. Doctors at Mayo Clinic developed a liquid meal program geared toward people who need to lose a lot of weight."
Facebook Friend Request - A young doctor gets a message from a dying patient
 From the NYTimes:
From the NYTimes: "Last winter, in the middle of my intern year, I became Facebook friends with a young man who was dying in the intensive-care unit. An investment banker in his mid-20s, he thought he was healthy until a fluttering in his chest and swollen ankles took him to a doctor. Now he was in the I.C.U. with a rare cardiac condition and the vague possibility of a transplant.
“Are you on Facebook?” he asked me. “I’ll friend you, and you can see the pictures.”
He’d been sending upbeat status updates from the I.C.U.; to read them, you’d never know he was so sick, but to me they were missives from a dying man."
Comments from Google Buzz:
Mark Hawker - Just before I do comment, I'd like to say that I do not have a clinical background so I cannot comment or empathise on the writer's clinical content or her situation. However, I can comment on my personal feelings about the story.
My reaction to this story was one of shock. A testosterone-filled medical student who got herself into a preventable situation. The lines that made me most uncomfortable were:
- "This boy on Facebook was, well, hot."
- "I didn’t think there was an ethical principle about following a patient on Facebook, and I didn’t worry that he’d see a picture of me in a bikini on my page."
It's not the fact that she didn't reply to this patient's message but the fact that she got herself into that situation in the first place. Would a doctor take a patient's telephone number to "see how they were" or go out bowling with them? Her emotions got the better of her and this led to more stress/turmoil in the future stages of the case. Does she feel this way to all her patients, or just the good-looking ones?
Secondly, "I signed on to our medical-records system and followed the notes that led — inevitably now — to his death." What now? In my opinion she had no right at all to do this. Her access was not about clinical care at all, nothing shy of being nosey. Does she also look up the medical notes of her ex-boyfriends etc.?
i just can't see how this would be OK? Maybe I'm missing the point... 10:51 am
“Are you on Facebook?” he asked me. “I’ll friend you, and you can see the pictures.”
He’d been sending upbeat status updates from the I.C.U.; to read them, you’d never know he was so sick, but to me they were missives from a dying man."
Comments from Google Buzz:
Mark Hawker - Just before I do comment, I'd like to say that I do not have a clinical background so I cannot comment or empathise on the writer's clinical content or her situation. However, I can comment on my personal feelings about the story.
My reaction to this story was one of shock. A testosterone-filled medical student who got herself into a preventable situation. The lines that made me most uncomfortable were:
- "This boy on Facebook was, well, hot."
- "I didn’t think there was an ethical principle about following a patient on Facebook, and I didn’t worry that he’d see a picture of me in a bikini on my page."
It's not the fact that she didn't reply to this patient's message but the fact that she got herself into that situation in the first place. Would a doctor take a patient's telephone number to "see how they were" or go out bowling with them? Her emotions got the better of her and this led to more stress/turmoil in the future stages of the case. Does she feel this way to all her patients, or just the good-looking ones?
Secondly, "I signed on to our medical-records system and followed the notes that led — inevitably now — to his death." What now? In my opinion she had no right at all to do this. Her access was not about clinical care at all, nothing shy of being nosey. Does she also look up the medical notes of her ex-boyfriends etc.?
i just can't see how this would be OK? Maybe I'm missing the point... 10:51 am
Ves Dimov, M.D. - I see your point and I think it's a valid one. We already know that some physicians have hard time looking at patients only from a professional point of view, and I agree with you that this is a problem. It has little to do with Facebook though since this mind set can be propagated through any communication channel. Facebook provides some misunderstood "privacy", if not anonymity. 11:04 am
Mark Hawker - Yes, that's right. Facebook is merely a "medium" much like telephone, an address, papyrus, etc.
I can't come to imagine how hard it must be to separate from a patient but can you be too human which can lead to enormous emotional stress in the long-term? Maybe this encounter led the writer to feel lonely about her own situation? Would she have reacted the same if she found that he was not single? Though, this is information she should never really have found out about...
Can this type of separation be taught, or is it embedded within us and cannot be taught? 11:11 am
Ves Dimov, M.D. - "Can you be too human?"
Yes. There are two rather simplistic schools of thought for professionals: cold and technical but gets the job done vs. warm and fuzzy, bubbly and compassionate... "When you have appendicitis, you want a surgeon, not a poet holding you hand for comfort."
"Can this type of separation be taught?"
I think so. It's part of the professionalism - one of the 6 core competencies of a physician training:
http://casesblog.blogspot.com/2008/03/remembering-acgme-6-core-competencies. 11:18 am
Anne Marie Cunningham - I think I did read this around the time that it was first posted on NYT... in fact I'm sure I did. At the time I was struck by how this doctor communicated her confusion over many things... not being able to help this patient... realising that he had a life before being a patient... struggling with his death. It didn't strike me that she had been unprofessional. She engaged in small talk with the patient and he invited her to be a friend on Facebook to see the photos of his trip. She could have said "No, I'm not on Facebook" or "No, I don't think it is appropriate to be friends with a patient on Facebook", but she didn't. Instead she allowed him to invite her to see those photos. We don't know how public his profile page was. Perhaps it was public. Maybe she shouldn't have looked again. But she did. With regards to following up his medical story through his notes... well I don't think this is inappropriate either. Looking at what happens to patients after you have looked after then is how you learn. It's what we encourage students to do and it absolutely the best way to learn when you are a doctor too. Should she have written this account? Well, through it... and I presume she has changed enough so that we couldn't figure out who the patient is.... we are given something to think about. We are able to think about what she should have done. We are able to think about what we would do if we are patients. This is a generous act because she is sure to know that some people will be critical. Most of the comments criticise her for not responding to this direct message and it is what she criticises herself for. Should she have gotter herself into this situation? Who knows. Would she do it again? Only she knows. I commented on twitter, that I don't think that her behaviour was unprofessional. That doesn't mean that I think it was professional. I think that she is struggling with a professional identity. That's not surprising because she is a very young doctor.
I'm not sure from reading this if she ever actually did become his friend on Facebook. Responding to a message allows people to see more of your profile, and it sounds as if that is why she made the remarks about the possibility or not of him seeing her in a bikini. Perhaps it wasn't something to worry about because there are no photos of her like that on Facebook. With regards to seeing him as 'hot', I take that she sees that in contrast to his lack of hotness in a hospital bed. She gets to see him as the well person he was before being a patient. It probably made the tragedy of his story, and the sadness of his situation even more real to her.
Should she not have known any of this? Some would say, as a few commenters do, that the sadness is that she only came to know about him as a whole person through Facebook. The nature of medicine is that we mostly only ever get to see our patients on our turf. Seeing and knowing about their whole lives, if they are happy for us to, is not wrong or innapropriate.
Medicine is not just about information. It is about caring and that is what this story tells us about. 7:08 pm
Anne Marie Cunningham - PS For a critique of 'professional distance' as professionalism I suggest this paper by Joanna Shapiro http://www.peh-med.com/content/3/1/10
No one ever said that being a doctor was easy! 7:14 pm
From Twitter:
@markhawker
Read this account... http://nyti.ms/dcM271 Do you think this is funny or very, very worrying? Do people think this article about a medical student and Facebook is funny? http://nyti.ms/bc80tC Maybe I'm getting too old for this...
Anyone care to count the number of ethical breaches that she abused in the story and, worryingly, admitted to. Would that happen in the UK?!
I'm still torn as to how "human" a doctor should be whilst working. Well, maybe one not driven entirely by testosterone. Yes, does require a lot of thought! I was just taken aback by the article & how the world seems to think these things are OK.
Confidentiality, looking up medical records unauthorised, wishing to respond to a "casual online message". Qualities of a Dr? Nothing catches your eye about testosterone-crazed medical students let loose to breach confidentiality regulations and ethics? You don't think that this student maybe got herself in too deep because of a hot-blooded crush which affected her clinical judgment? Would she give him a phone number etc.? Has the ICU been mistaken for a bar?! Is there a difference between being human and emotional?
It's not the fact she didn't communicate, it's the fact she got herself into that position in the 1st place.
"This well-intentioned resident naively violated HIPAA by accessing records for no purpose other than her own personal interest." Thank you.
There are many factors that contribute to this: personal, age, experience etc. I think her "issue" was preventable.
Interested in learning about the psychological effects of these interactions and skeptical about the altruism of the writer.
Interested to hear your thoughts. I think the article is wrong in many ways... Will watch out for your analysis.
I wonder if she removed him as a Facebook friend... If not, I could find his name, right? Not too anonymous.
Note:
If you see your comment here and you would like to have it removed, please let me know via comment or email and I will comply with your request within the same business day.
Lives - Friend Request - NYTimes.com.
Image source: Wikipedia.
Tuesday, April 13, 2010
Australian grandmother beats off attacking shark - BBC
From BBC:
"An Australian grandmother has survived a shark attack by repeatedly punching and kicking the animal after it "ripped off" part of her body.
Surgeon Mark Flanagan said: "We can estimate that she lost about 40 per cent of her blood volume from the degree of shock that she had when she came in, and the fact that we required to give her several units of blood."
Mrs Trumbull said she was happy to be alive."
Shark Tunnel and Aquarium at Omaha Zoo, Nebraska.
"An Australian grandmother has survived a shark attack by repeatedly punching and kicking the animal after it "ripped off" part of her body.
Surgeon Mark Flanagan said: "We can estimate that she lost about 40 per cent of her blood volume from the degree of shock that she had when she came in, and the fact that we required to give her several units of blood."
Mrs Trumbull said she was happy to be alive."
Shark Tunnel and Aquarium at Omaha Zoo, Nebraska.
How to use Google Docs Drawings for medical mind maps
Google Drawings is a new collaborative drawing editor - part of the updated Google Docs. It is free to use, just like the rest of Google Docs. The new standalone drawings editor lets you collaborate in real time on flow charts, designs, diagrams and other fun or business graphics. You can copy these drawings into documents, spreadsheets and presentations using the web clipboard, or share and publish drawings just like other Google Docs.
Until now, my service of choice for medical mind maps was Bubbl.us and I have made more than 100 diagrams with it for AllergyCases.org:
Mind Map Diagrams in Allergy and Immunology
Bubbl.us works very well but I was concerned about embedding the mind maps in case the service goes down temporarily or if the company closes down in the future (mind maps can be exported in XML format for backup). None of these should be a problem with Google Docs. Drawings is obviously behind Bubbl.us in terms of features but it works for basic mind maps and I am planning to use it frequently in the future.
You can embed the minds maps as images, just like you do with YouTube videos, or provide a link to the original mind map and share it for collaboration:
Example: Accidental Injection of Epinephrine Into Finger
Every time you update the mind map in Google Docs/Drawings, the image updates too.
See a few mind maps created with Drawings below:

Until now, my service of choice for medical mind maps was Bubbl.us and I have made more than 100 diagrams with it for AllergyCases.org:
Mind Map Diagrams in Allergy and Immunology
Bubbl.us works very well but I was concerned about embedding the mind maps in case the service goes down temporarily or if the company closes down in the future (mind maps can be exported in XML format for backup). None of these should be a problem with Google Docs. Drawings is obviously behind Bubbl.us in terms of features but it works for basic mind maps and I am planning to use it frequently in the future.
You can embed the minds maps as images, just like you do with YouTube videos, or provide a link to the original mind map and share it for collaboration:
Example: Accidental Injection of Epinephrine Into Finger
Every time you update the mind map in Google Docs/Drawings, the image updates too.
See a few mind maps created with Drawings below:
In order to publish the mind map diagram on the web, you have to click the "Share" button in the top right corner of the Google Docs menu. After the diagram is published, you will see the options to embed the image with different sizes and the link to share the original drawing with options to be edited by collaborators.
Getting started guide for Google Drawings
Can images (mind maps, infographics) stop data overload? Symptom of the computer age: overwhelmed, we delay decisions http://goo.gl/URMKm
Can images (mind maps, infographics) stop data overload? Symptom of the computer age: overwhelmed, we delay decisions http://goo.gl/URMKm
University of Cambridge shows high-resolution Newton notebooks online. He used mind maps - check Trinity College Notebook, image 5.
Comments from Twitter:
Robbo @BiteTheDust: excellent. will give it a go RT @DrVes: How to use Google Docs Drawings for medical mind maps bit.ly/J4BX7U
Comments from Twitter:
Robbo @BiteTheDust: excellent. will give it a go RT @DrVes: How to use Google Docs Drawings for medical mind maps bit.ly/J4BX7U
Monday, April 12, 2010
Health experts' tips for safe international travel
CDC video: Health experts suggest that you take several key steps to be protected against injury or illness when travelling to developing nations. This includes packing a health kit, bringing medications, and getting immunizations for safe and healthy travel.
Johns Hopkins Medicine podcast now has a blog
 The weekly podcast by Johns Hopkins Medicine now has a blog hosted for free at Blogger.com by Google:
The weekly podcast by Johns Hopkins Medicine now has a blog hosted for free at Blogger.com by Google:http://hopkinspodblog.blogspot.com
I have been a regular listener for years and have found the podcast to be both educational and enjoyable - not a common combination.
The weekly podcast looks at the top medical stories of the week for people who want to become informed participants in their own health care. The presenters are Elizabeth Tracey, director of electronic media for Johns Hopkins Medicine, and Rick Lange M.D., professor of medicine at Johns Hopkins and vice chairman of medicine at the University of Texas Health Science Center at San Antonio.
I have been a regular listener for years and have found the podcast to be both educational and enjoyable - not a common combination.
The weekly podcast looks at the top medical stories of the week for people who want to become informed participants in their own health care. The presenters are Elizabeth Tracey, director of electronic media for Johns Hopkins Medicine, and Rick Lange M.D., professor of medicine at Johns Hopkins and vice chairman of medicine at the University of Texas Health Science Center at San Antonio.
Image source: Johns Hopkins
Sunday, April 11, 2010
29 Debates About the "Right Way" to Blog
 ProBlogger collected 29 Debates Bloggers Have about Blogging. Some of my responses are listed below, see ProBlogger's site for the complete list. Please share your thoughts in the comments.
ProBlogger collected 29 Debates Bloggers Have about Blogging. Some of my responses are listed below, see ProBlogger's site for the complete list. Please share your thoughts in the comments.RSS Feeds - Full vs Partial Feeds
- My opinion: Full feed.
Comment Sections – Comments vs No Comments
- Comments always open.
Post Frequency – Post More vs Post Less
- Short posts daily.
How Many Blogs? – Focus upon One Single Blog vs Having Many Smaller Blogs.
- I have 3-4 blogs.
Domain Names – long vs short, hyphens vs non hypens, .com vs other extensions (like .net, .org), local vs global domain extensions
- Short names, free domain names by Blogger.com.
Hosting – hosted vs self hosted
- Hosted by Blogger.com.
Post Titles – descriptive vs keywords
- I use natural language post titles - descriptive.
Content – Link content vs Original content
- Mostly links and comments, I wish I had more time to write long-form original content.
Design – Professional Design vs Templates
- I modify the templates to create my "own" designs. It's quite enjoyable actually.
Ownership – Use Social Media vs Build Your own properties
- I think your blog should be your "home" on the web.
Post Length – Long in Depth Posts vs Short, Sharp Posts
- Again, I wish I had the time to write long posts but I don't.
Topic – Niche vs Broad Topics
- Niche topic blogs work better.
Blogger Name – Anonymous blogging vs Using Your Name
- Using your name is a much better approach for medical bloggers.
Subscribers – RSS is Best vs Email is Best
- I like RSS better.
SEO – Writing for Search Engines vs Writing for Humans
- I write for humans only.
Personal Blogging – Sticking to Topic vs Injecting Personality and Personal details
- I try to write objectively from a scientific perspective. Personal stories are probably better suited for a paper diary.
Comment Moderation – Highly Regulated and Moderated vs Anything Goes
- I moderate all comments and delete all self-promotional and possibly offensive material.
Social Media vs Search – focus upon social media rather than search engines as traffic sources
- If you write quality content, Google will find you.
LinkBait – Anything goes (e.g.. Personal Attacks) vs Strong Boundaries Around What is and Isn’t Acceptable
- I don't use link baits and I have never posted anything even close to a personal attack on my blogs.
Bloggers Participation in Comments – Respond to Every Single Comment vs Let Readers Talk to Each Other and Don’t Interact
- I don't feel compelled to respond to every single comment. Let readers interact.
This Google video shows that it takes about 2 minutes to start a blog on Blogger.com. Creating a web site has never been easier.
References:
29 Debates Bloggers Have about Blogging. ProBlogger, 2010.
Saturday, April 10, 2010
"Europeans Work to Live and Americans Live to Work" But Who is Happier?
 Americans work 50% more than the Germans, the French and the Italians. Americans may work more than Europeans because of domestic tax rates - there are lower tax rates in the US than in Europe, and hence working more pays off more in the US. In other words, working longer hours pays off more in the US than in Europe.
Americans work 50% more than the Germans, the French and the Italians. Americans may work more than Europeans because of domestic tax rates - there are lower tax rates in the US than in Europe, and hence working more pays off more in the US. In other words, working longer hours pays off more in the US than in Europe.This study compares the working hours and life satisfaction of Americans and Europeans using the World Values Survey, Eurobarometer and General Social Survey.
The purpose is to explore the relationship between working hours and happiness in Europe and America. Is it possible that working more makes Americans happier than Europeans?
The findings suggest that Americans may be happier working more because they believe more than Europeans do that hard work is associated with success.
References:
Europeans Work to Live and Americans Live to Work (Who is Happy to Work More: Americans or Europeans?). Adam Okulicz-Kozaryn. Journal of Happiness Studies, 2010.
Image source: Wikipedia, GNU Free Documentation License.
{kind=link}
Friday, April 9, 2010
Jamie Oliver at TED: Teach every child about food
Sharing powerful stories from his anti-obesity project in Huntington, W. Va., TED Prize winner Jamie Oliver makes the case for an all-out assault on our ignorance of food.
Why Twitter may not be good enough for scientific information and discussion
 I appreciate the re-tweet below but I did not say anything remotely close to this sentence:
I appreciate the re-tweet below but I did not say anything remotely close to this sentence:@sevinfo Reading "top" journals only distorts your world - Argument for scrapping peer review at BMJ blogs via @DrVes & @KentBottles
http://twitter.com/sevinfo/status/10929698882
My original tweet:
@DrVes The naïve concept that the “top journals” publish the important stuff and the lesser journals the unimportant http://goo.gl/utJ5
http://twitter.com/DrVes/status/10892767666
My expanded citation on Google Buzz:
The false idea that only the “top journals” publish the important stuff
From the former Editor-in-Chief of BMJ:
The naïve concept that the “top journals” publish the important stuff and the lesser journals the unimportant is simply false. People who do systematic reviews know this well. Anybody reading only the “top journals” receives a distorted view of the world. Unfortunately many people, including most journalists, do pay most attention to the “top journals.”
http://blogs.bmj.com/bmj/2010/03/22/richard-smith-scrap-peer-review-and-beware-of-%E2%80%9Ctop-journals%E2%80%9D/
http://www.google.com/buzz/110859855629071891085/TPmyVKjvZS9/The-false-idea-that-only-the-top-journals-publish
Please click the Buzz link above to see how much more "richer" the comments there are as compared to Twitter where the microblog updates (tweets) are limited to 140 characters.
This little example adds to the opitinion that many times Twitter is not good enough for scientific information and discussion.
Follow-up:
@sevinfo: yoicks! I was agreeing to need to read both "top" & less exciting ; not saying that reading science distorts your world! For record - @DrVes points out that text on last link open to misinterpretation - Keep reading science journals both top & less glamourous!
Comments from Google Buzz (March 23-24):
Kathy Mackey - Appreciate the followup Dr. Ves. I read the article yesterday on BMJ on scientific journals and felt I was missing something. It is true that 140 characters can be difficult to relay important information to the public
Brian Ahier - This is a problem that can not be adequately addressed because of the character limitation in Twitter. But it is an opportunity for a service like Buzz to be a bridge for longer commentary and discussion. I suggest we have more conversations in Buzz and then tweet a link to the post.
Ves Dimov, M.D. - Agree. Works very well with some posts. However, the Buzz adoption rate is significantly lower than Twitter and seems to have plateaued a few week after its launch.
Brian Ahier - Quality vs. Quantity?
I have found a much higher quality conversation seems to be happening on Buzz. Perhaps some of the adoption will not be missed. I have yet to be bothered by a spam account on Buzz and many of the followers on Twitter soon become inactive.
Ves Dimov, M.D. - True. People put more thought into Buzz comments - the accounts are often tied to their "real" identity after all. Participation fatigue is a common occurrence among all services.
Brian Ahier - I am also fortunate that many of my higher profile followers like Tim O'Reilly, Richard MacManus, and Robert Sconle are active on Buzz. As Buzz matures I think we will see some interesting applications. Then when Google buys Twitter we'll be all set ;-)
Ves Dimov, M.D. - Yes. Although Evan Williams keeps saying that Twitter is not for sale not matter what the price...
Brian Ahier - Yeah, Ev is an idealist :-D
Ves Dimov, M.D. - You have to respect the guy - he brought two very important services to popularity and success - Blogger and Twitter. Even one would be enough for the Internet history books... :)
Ves Dimov, M.D. - @Brian Ahier - I'm sorry I deleted your comment by mistake and there is no "Undo" in Buzz. "You" was meant in general not for you in person. And, yes, I share the same opinion.
Brian Ahier - Buzz does need an undo - but as I said, I admire people who old to their ideals. Ev has made some outstanding contributions and has an amazing talent.
Neil Mehta - Some of my best online experiences have been on Buzz - feels like a civilized sit down dinner with a conversation. Twitter can leave one feeling like everyone is rushing around on a big field shouting "hello" to the world, hoping someone will reply and start a conversation - it is great when to find that stranger with whom you share an interest but that happens rarely and the conversation is usually very unsatisfactory. Understand the Twitter functionality was not designed for conversations......
Vamsi Balakrishnan - @Neil Mehta: It's exactly as Dr. Ves said though; Buzz is tied to your real identity more or less, which is especially true for those who have verified profiles. It's also easier to have conversations since there's no 140 character limit...and it goes to those who use twitter anyway if you've enabled it. So, for me at least, it was a seamless transition.
The only problem that exists though, which truth be told hasn't affected me yet, is that there's a 300 comment limit. 300 replies to a post can exist, no more.
Thursday, April 8, 2010
Are doctors ready for virtual visits? Telemedicine may not be accurate enough
Are Doctors Ready for Virtual Visits? Many fear telemedicine will jeopardize the doctor-patient bond. NYT http://bit.ly/7c2RA8Telemedicine has a place for second opinion when initiated by a physician but primary assessment is more problematic. One successful example of telemedicine is Cleveland Clinic's second opinion service for physicians abroad. For reference, please see our blog post from a few years ago: Cleveland Clinic Offers a Second Opinion Online for $565 http://bit.ly/4NQyer
The accuracy of teledermatology was inferior to real-life clinic dermatology for melanoma diagnosis http://bit.ly/8A4oiu.
CNN Video: Doctor will see you now -- on Webcam. Telemedicine takes a new turn. Now you can see the doctor while you shop, as CNN's Elizabeth Cohen reports.
Related:
Melanoma - JAMA Patient Page illustrates the ABCDE of diagnosis, 2011.
Skin cancer in the USA - follow Australia's successful "Slip Slop Slap Seek Slide" campaign - The Lancet, 2011.
Telemedicine boosting dermatology care: improved outcomes, with better diagnosis and disease management. AMA News, 2012.
Skin cancer in the USA - follow Australia's successful "Slip Slop Slap Seek Slide" campaign - The Lancet, 2011.
Telemedicine boosting dermatology care: improved outcomes, with better diagnosis and disease management. AMA News, 2012.
Martina Navratilova Fighting Breast Cancer - ABC Video
In February 2010, the tennis legend was diagnosed with an aggressive form of ductal carcinoma in situ (DCIS), considered the earliest form of breast cancer. Navratilova had a lumpectomy in February, during which her doctors determined that the cancer had not spread to her lymph nodes. She says there is only a "very small chance of it coming back."
Navratilova's cancer was diagnosed during a routine mammogram, after not having one for four years, and she hopes that speaking out will inspire other women to get mammograms.
"The reason I wanted to speak about this is to encourage these woman to have mammograms," she said. "I just want to encourage women to have that yearly check-up."
References:
Martina Navratilova Fighting Breast Cancer
Wednesday, April 7, 2010
Eradication of nasal colonization with S. aureus associated with a decrease in postoperative surgical-site infections
Nasal carriers of Staphylococcus aureus are at increased risk for health care–associated infections with this organism.
Eradication of colonization with S. aureus by screening at admission and subsequent decolonization (with intranasal mupirocin and chlorhexidine skin washes) were associated with a decrease in postoperative surgical-site infections.
In a randomized, double-blind, placebo-controlled trial, S. aureus nasal carriers were treated with mupirocin nasal ointment and chlorhexidine soap.
A total of 6771 patients were screened on admission, 1270 nasal swabs from 1251 patients were positive for S. aureus. All the S. aureus strains identified on PCR assay were susceptible to methicillin and mupirocin.
The rate of S. aureus infection was 3.4% in the mupirocin–chlorhexidine group, as compared with 7.7% in the placebo group (relative risk of infection, 0.42). The effect of mupirocin–chlorhexidine treatment was most pronounced for deep surgical-site infections (relative risk, 0.21).
References:
Preventing Surgical-Site Infections in Nasal Carriers of Staphylococcus aureus. NEJM, 1/2009.GIANTmicrobes in Toys & Games section of Amazon.com http://goo.gl/gMrf
Scaring physicians away from using social media
This useful critical review by a freelance journalist at the NEJMJobs site has a focus on some of the litigation risks inherent to the use of social media in healthcare:
http://www.nejmjobs.org/career-resources/social-media-and-physicians.aspx
"Dr. Pho, who spends up to three hours a day in social media activities, is surely in a minority of physicians who devote considerable time to blogging, Twittering, or engaging in Facebook updates.
Social Media Activity Risks Difficult to Predict
Despite the potential professional benefits of social networking participation, some physicians are approaching the social media realm with trepidation, for fear that personal and professional presences will overlap in a manner that increases liability exposure.
That’s a valid concern, because the medico-legal aspect of social media activities has been little explored and is not well understood. In addition, the obvious risks of incurring HIPAA violations should patients’ health information be unwittingly exposed are a deterrent. “The laws haven’t caught up with social media and networking, so to be safe I don’t blog about my patients,” Dr. Pho said. “Even though I think that interesting or challenging cases can be used as a learning tool, too much of my professional livelihood is at stake.”
None of the physicians interviewed for this article have accepted patients’ requests to become Facebook friends, and all cited concerns that doing so would “cross the boundary” between a personal and professional relationship.
"I think that very few doctors are interacting with patients directly on Facebook because we’re so terrified of being accused of practicing medicine and getting sued. Whatever you type is eternal and a perfect record of whatever you said,” she said. “That makes it all even more scary.”
“We’re concerned about this because there have been instances in which physicians have used Facebook in an inappropriate manner,” said David Troxel, MD, The Doctors Company’s medical director. “Social media networks are not HIPAA compliant and are just not appropriate for any physician-patient communication, so it’s a real liability threat because it’s so easy to lapse into a casual conversation.”
The NEJMJobs article linked in the paragraph above does not discuss the use of social media for medical education of students, residents and patients.
Another area that was not highlighted enough was the widespread use of Facebook "fan pages" by hospitals and physicians to attract patients and create relationships. Does this mean that the patients can be "your fans" but not "your friends"?
Overall, this article is a good review of some of the risks involved with the social media adoption in healthcare.
However, for a more nuanced approach to social media use by physicians, please review this detailed primer by the cardiologist Dr. Wes:
http://drwes.blogspot.com/2010/03/for-cardiologists-twitter-primer.html
Related:
Facebook Friend Request - A young doctor gets a message from a dying patient - NYTimes, 2010.
Social Media Raise Liability, Ethical Questions for Doctors as Internet is challenging traditional boundaries. Boston Globe, 2010.
Image source: OpenClipArt.org, public domain.
Updated: 04/13/2010
Tuesday, April 6, 2010
How To: Getting Smart During Your Daily Commute
"The average American spends a good 100 minutes per day commuting to and from work. That amounts to about 433 hours per year! Now imagine using that time to learn something new — to read a great book, to take a class from a top university, to learn a new language.
We highlight our free audio resources that will maximize your drive time. Before getting started, make sure you have a big mp3 player and a way to listen to your mp3 player over your car speakers."
References:
Getting Smart During Your Daily Commute | Open Culture
Related:
We highlight our free audio resources that will maximize your drive time. Before getting started, make sure you have a big mp3 player and a way to listen to your mp3 player over your car speakers."
References:
Getting Smart During Your Daily Commute | Open Culture
Related:
How does clinical evidence work?
Ben Goldacre's Moment of Genius on BBC4 radio:
"Clinical trials in medicine are designed to be free from bias. They test, as objectively as possible, the effectiveness of a particular intervention.
When you bring the results of all these individual trials together, however, how do you weigh up what evidence is relevant and what is not? In 1993, a method of "systematic review" was introduced that enables us to get the clearest possible view of the evidence."
Subscribe to:
Posts (Atom)