 Chronic obstructive pulmonary disease (COPD) is a chronic disorder with high mortality rates (one of the top 5 causes of death).
Chronic obstructive pulmonary disease (COPD) is a chronic disorder with high mortality rates (one of the top 5 causes of death).COPD is expected to rise to the third leading cause of death worldwide by 2030. More than 25% of COPD patients have never been smokers.
Some important controversies in COPD management still exist:
- The classic way to define COPD has been based on spirometric criteria, but more relevant diagnostic methods are needed that can be used to describe COPD severity and comorbidity
- Initiation of interventions earlier in the natural history of the disease to slow disease progression is debatable
- There are controversies about the role of inhaled corticosteroids (ICS) in the management of COPD
- Long-term antibiotics for prevention of exacerbation have had a resurgence in interest
New drugs are urgently needed for management of COPD exacerbation.
COPD is a complex disease and consists of several phenotypes that in future would guide its management.
Asthma Inhalers (click to enlarge the image). Advair and Symbicort are FDA-approved for treatment of COPD in the U.S.
References:
Controversies in treatment of chronic obstructive pulmonary disease. Prof Klaus F Rabe MD a , Jadwiga A Wedzicha MD b. The Lancet, Volume 378, Issue 9795, Pages 1038 - 1047, 10 September 2011.
New insights into the immunology of chronic obstructive pulmonary disease. The Lancet, Volume 378, Issue 9795, Pages 1015 - 1026, 10 September 2011.
COPD—more vigorous research needed. The Lancet, Volume 378, Issue 9795, Page 962, 10 September 2011.
Diagnosis and Management of COPD - Current Guidelines
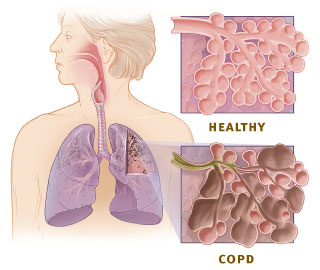
Image source: Enlarged view of lung tissue showing the difference between healthy lung and COPD, Wikipedia, public domain.


{kind=link}
{kind=link}